Multidisciplinary Rehabilitation Involving Endodontic Retreatment and Implant Planning
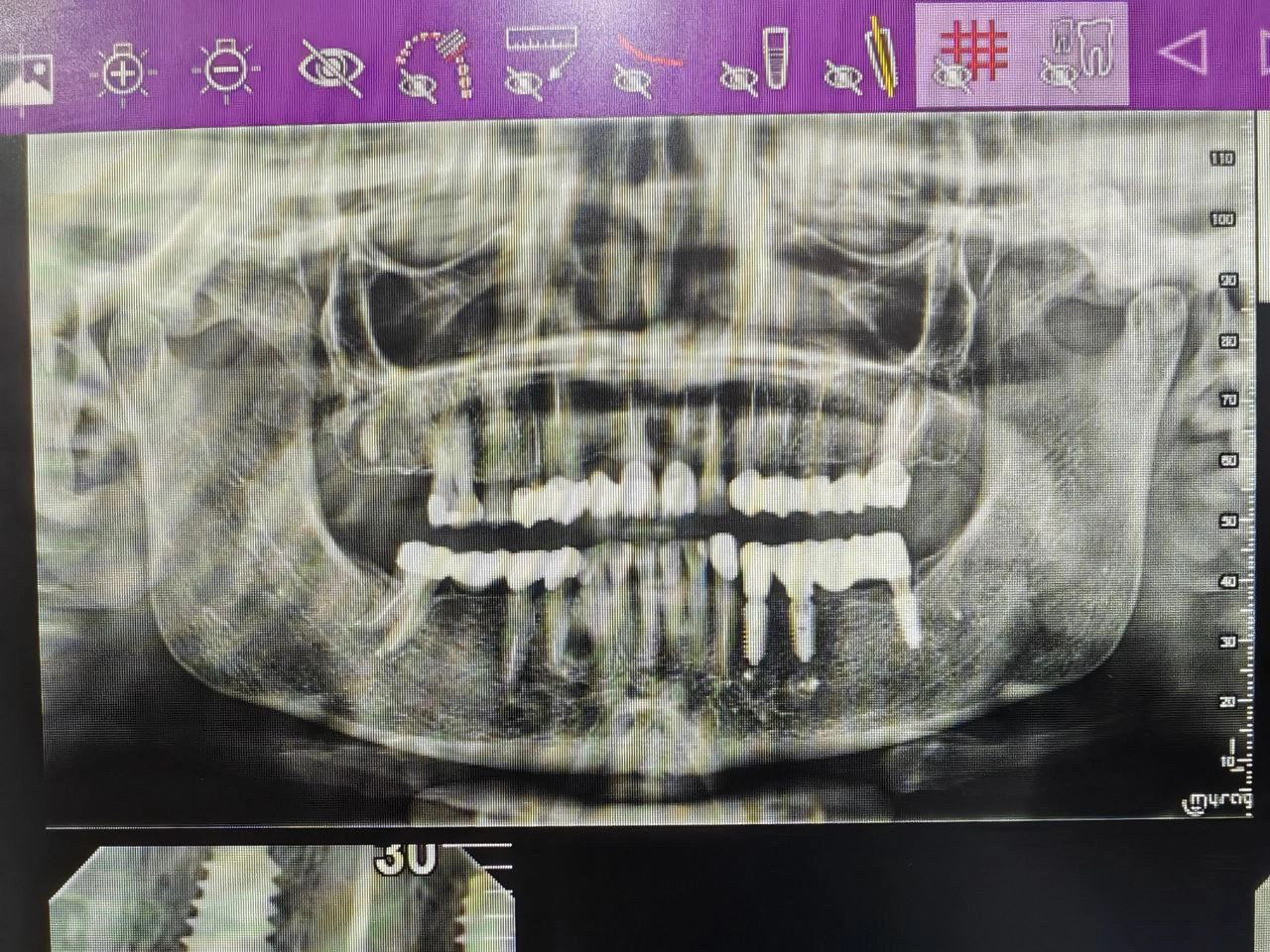
Pre-treatment panoramic view showing multiple endodontically treated teeth and bone levels prior to rehabilitation.
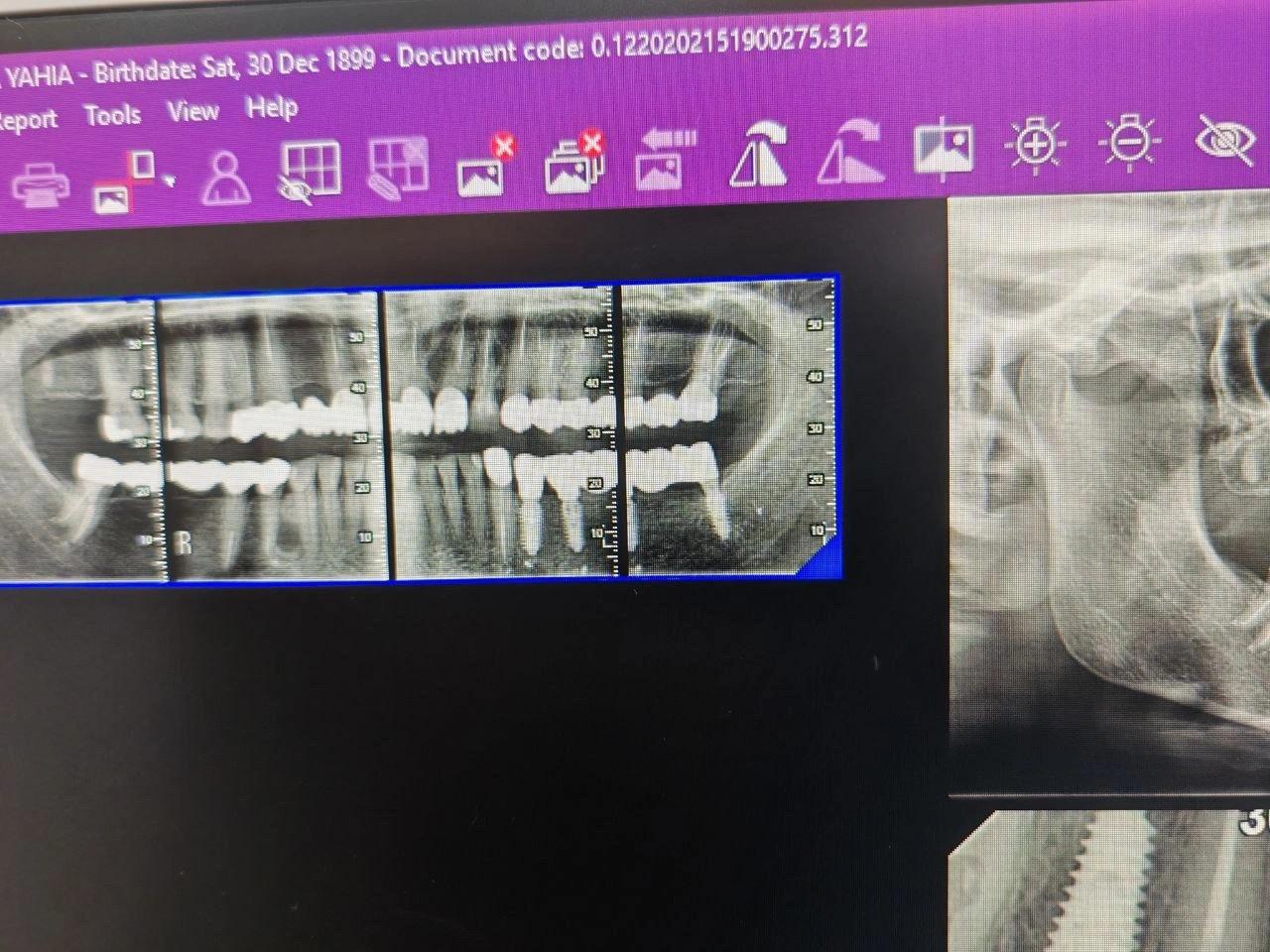
Pre-treatment CBCT slice showing periapical radiolucency associated with previously treated tooth.
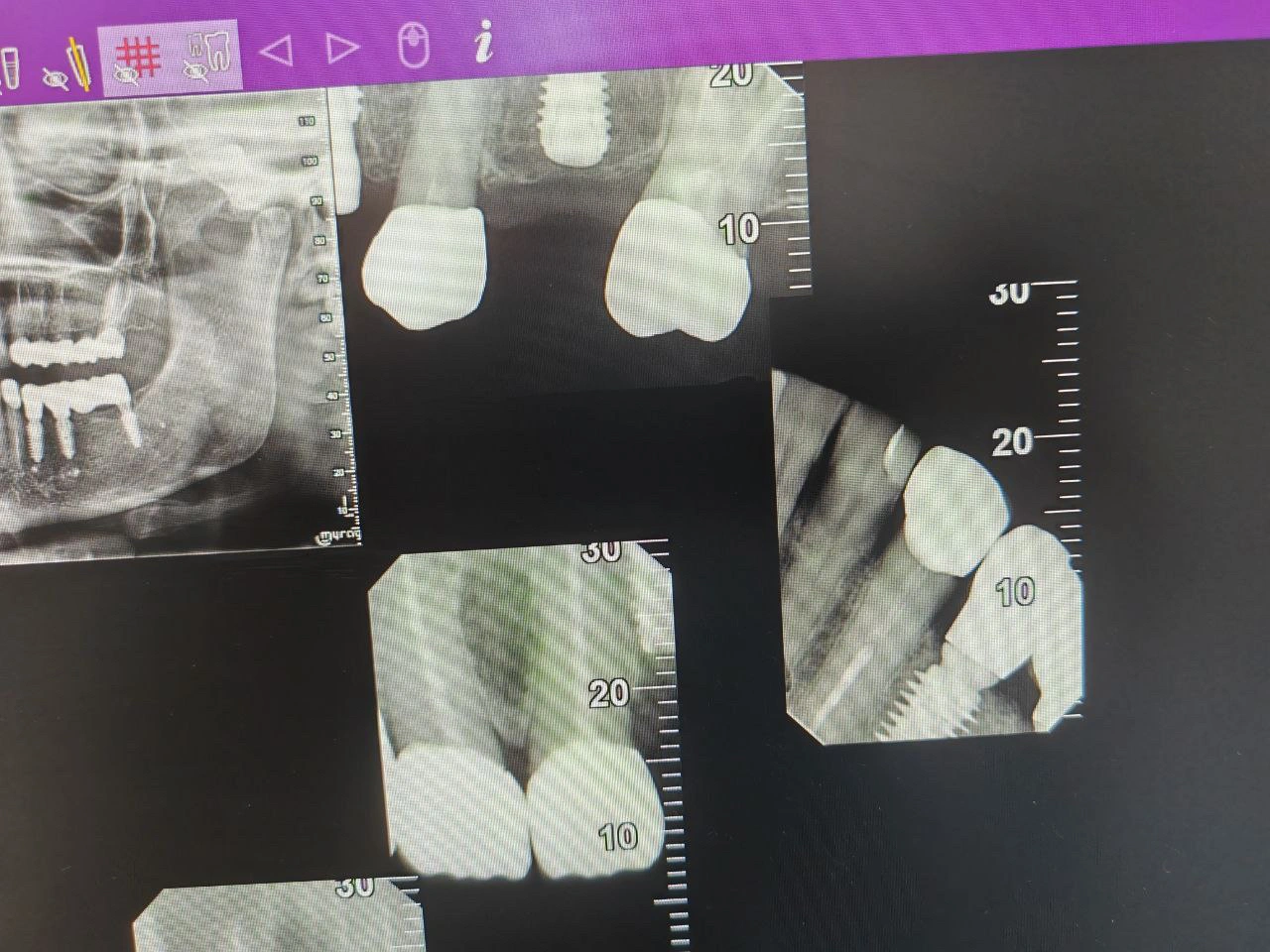
Post-endodontic retreatment periapical radiograph showing dense obturation and initial healing of periapical lesion.

Post-treatment panoramic radiograph showing final restorations and stable bone levels around implants.
Diagnosis
Radiographic Findings:
Periapical radiolucency associated with previously treated teeth, suggesting endodontic failure.
Presence of old crowns and posts with possible root fractures.
Multiple missing posterior teeth with adequate bone height for future implant placement.
Residual infection at the apex of endodontically treated teeth.
Clinical Findings:
Missing Ferrule effect
Tenderness on percussion in upper premolar and molar regions.
Compromised restorations with poor marginal seal.
Satisfactory oral hygiene, but localized gingival inflammation around old crowns.
Diagnosis:
Combined endodontic and prosthodontic failure, requiring retreatment and partial implant-supported restoration.
Treatment Objectives
Eliminate periapical infection via endodontic retreatment.
Restore missing teeth with implant-supported crowns.
Replace failing prosthetic restorations with new fixed units.
Achieve full function and esthetics while preserving natural teeth when possible.
Treatment Plan
Step 1: Cone-beam CT (CBCT) evaluation and periapical radiographs for root morphology and lesion extent.
Step 2: Removal of old restorations and posts, followed by root canal retreatment and obturation.
Step 3: Extraction of non-restorable teeth.
Step 4: Guided implant placement after healing period.
Step 5: Fabrication of new crowns and bridges, ensuring occlusal harmony.
Step 6: Final panoramic evaluation and follow-up.
Clinical Procedure Summary
Endodontic Retreatment: (Done by Endodontist)
Old gutta-percha removed, canals cleaned, shaped, and obturated.Radiographic Verification:
Periapical images confirmed dense, uniform obturation.Implant Phase: (Done by Implantologist)
Implants placed in posterior areas under local anesthesia; healing abutments placed after osseointegration.Prosthodontic Phase:
New fixed restorations fabricated and cemented; occlusion verified.
Results
Successful elimination of periapical lesions.
Functional occlusion re-established with implant and tooth-supported restorations.
Radiographic evidence of bone healing and stable implant integration.
Patient reported comfort and improved masticatory efficiency.
Discussion
This case demonstrates how interdisciplinary coordination between endodontics and prosthodontics ensures long-term success.
Radiographic follow-up is critical to verify periapical healing and implant osseointegration.
Reflection / Learning
Use of CBCT improves detection of missed canals and periapical pathology.
Sequential treatment (endodontic first, implant later) reduces complications.
Restorative design should consider load distribution between implants and natural teeth.