Root canal Treatment for tooth #32

Baseline sectional panoramic radiograph showing multiple implant-supported restorations with stable bone levels.
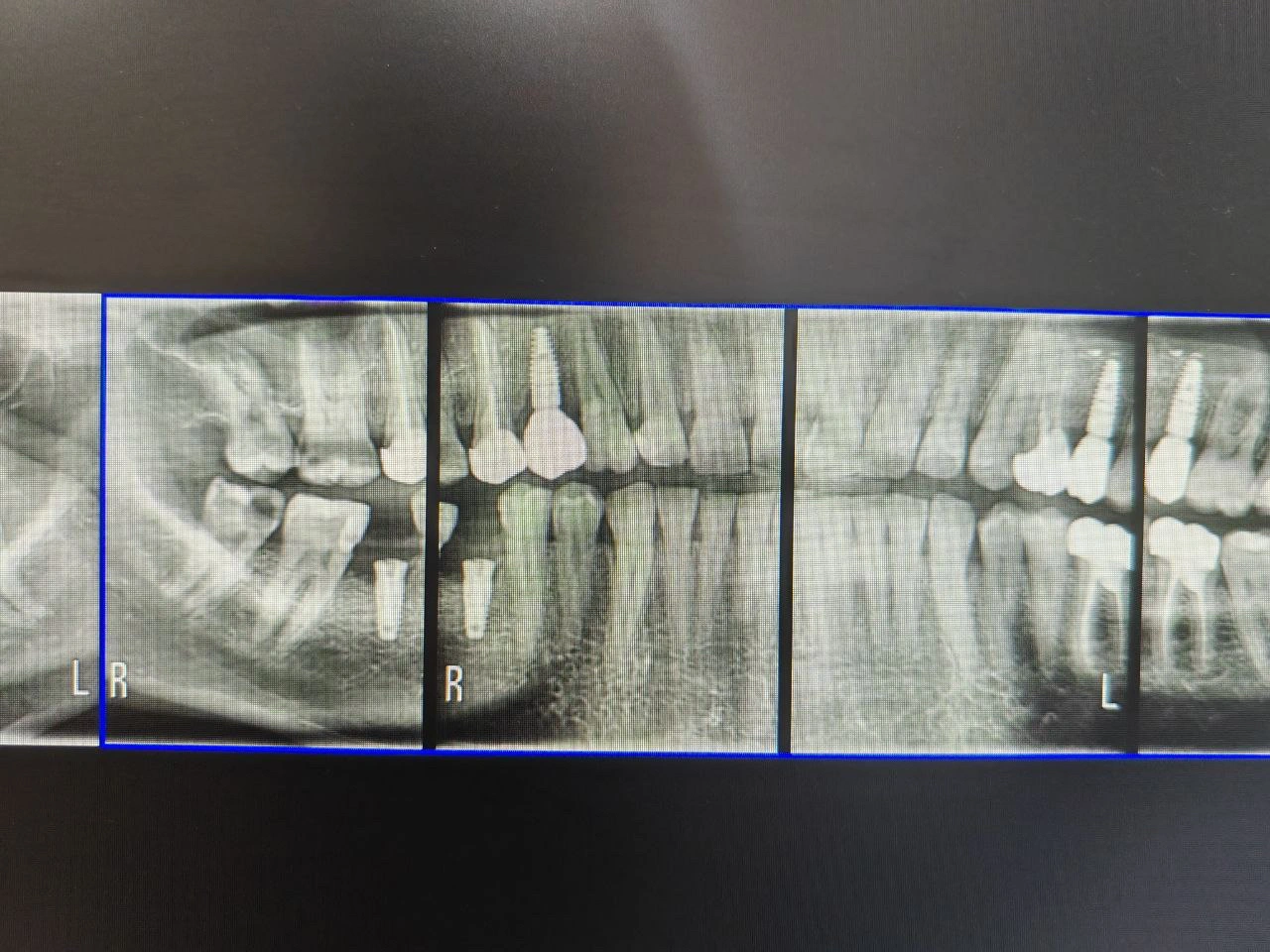
Follow-up sectional panoramic radiograph confirming maintained osseointegration and healthy bone margins around all implants.
Diagnosis
Radiographic Findings:
RL reaching the Pulp of tooth #32
Clinical Findings:
smooth surface caries reaches the pulp #32
Diagnosis:
Irreversible pulpitis
Treatment Objectives
Eliminate pulpal inflammation and disinfect the canal.
Relieve pain and associated symptoms.
Promote healing of periapical tissues.
Preserve the tooth in function and aesthetics.
Achieve a hermetic canal seal.
Restore tooth structure and prevent fracture.
Ensure long-term periapical health and function.
Treatment Plan
Step 1: X-ray
Step 2: Clinical evaluation
Step 3: Root Canal Treatment
Step 4: Restore tooth with Zirconia Crown.
Step 5: Follow-up recall after 6–12 months.
Clinical Procedure Summary
1. Diagnosis and Treatment Planning
Clinical and radiographic examination to confirm pulpal and periapical status.
Determine working length and canal morphology.
Obtain informed consent.
2. Access and Canal Preparation
Administer local anesthesia.
Prepare access cavity with proper straight-line access.
Determine working length using apex locator and confirm radiographically.
Clean and shape the canal using hand or rotary instruments with irrigation (NaOCl, EDTA, saline).
3. Obturation
Dry the canal with paper points.
Obturate with gutta-percha and sealer using the lateral condensation technique.
Verify obturation radiographically.
Seal the access cavity with a temporary.
4. Post-Endodontic Restoration and Crown Preparation
Remove temporary filling and assess remaining tooth structure.
Place a core buildup (composite).
Prepare the tooth for a full-coverage crown with proper finish line and taper.
Take final impression or digital scan.
Fabricate and cement a provisional crown.
5. Crown Cementation
Try-in the final crown for fit, occlusion, and aesthetics.
Cement permanently using resin.
Verify margins and occlusion.
6. Follow-Up
Schedule recall visits for clinical and radiographic evaluation of periapical healing and crown integrity.
Results
Tooth #32 became asymptomatic with resolution of pain and tenderness.
Radiographic evidence of periapical healing was observed.
The tooth was functionally restored with a full-coverage crown, providing good aesthetics and occlusal harmony.
No signs of reinfection or mobility were noted at follow-up.
Reflection / Learning
Reinforced the importance of accurate working length determination and thorough canal disinfection for long-term success.
Learned to maintain proper isolation and aseptic technique throughout treatment.
Gained experience in achieving an ideal coronal seal and selecting an appropriate post-endodontic restoration.
Understood the significance of timely crown placement to prevent fracture and reinfection.