RCT #18

Pre-Operative PA
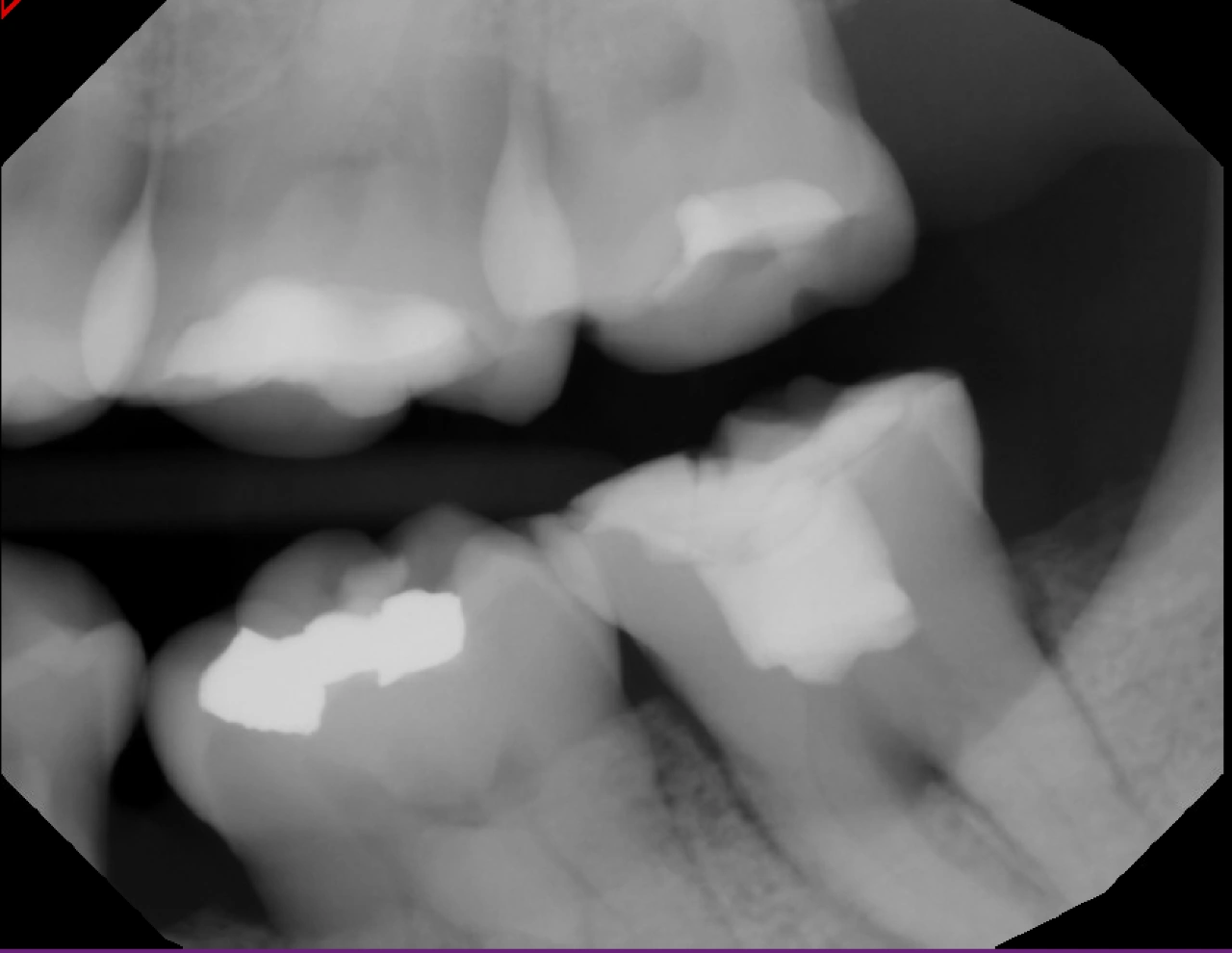
Pre-Operative Bitewing
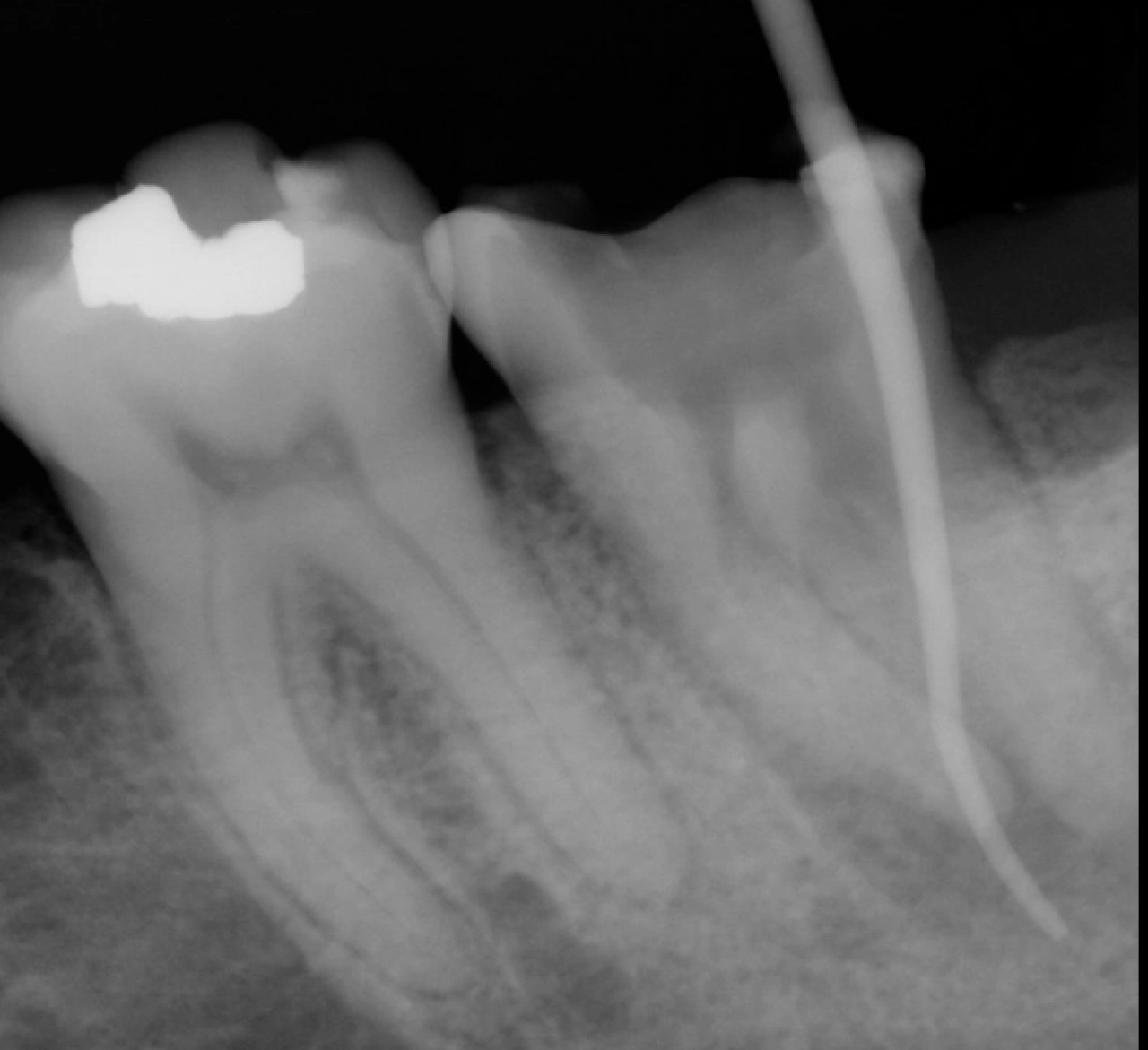
Sinus Tract Tracing First Visit
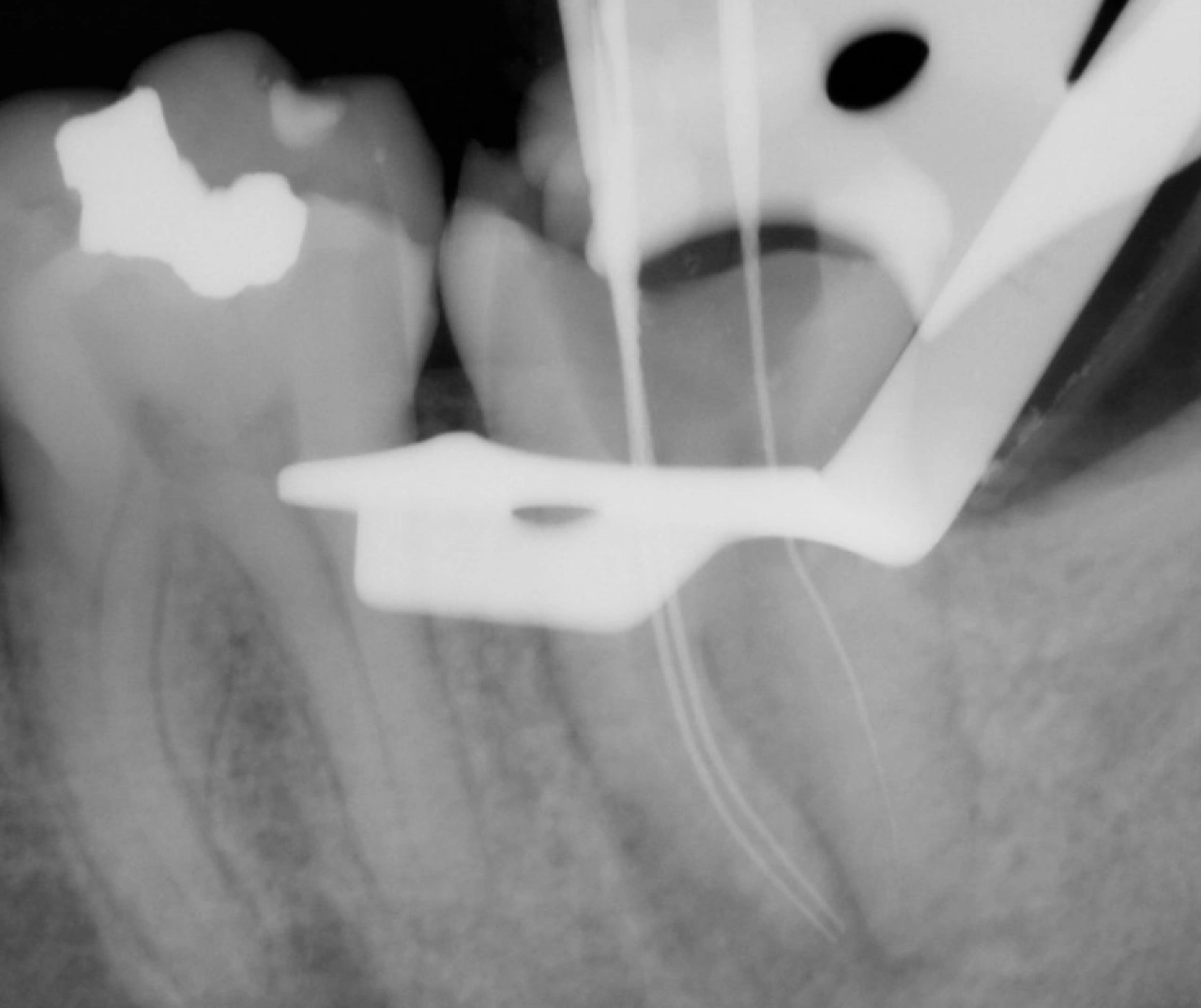
Working Length

IRM Placed

Second Visit: Sinus Tract Still Present

MTA Applied to reinforce internal fracture lines

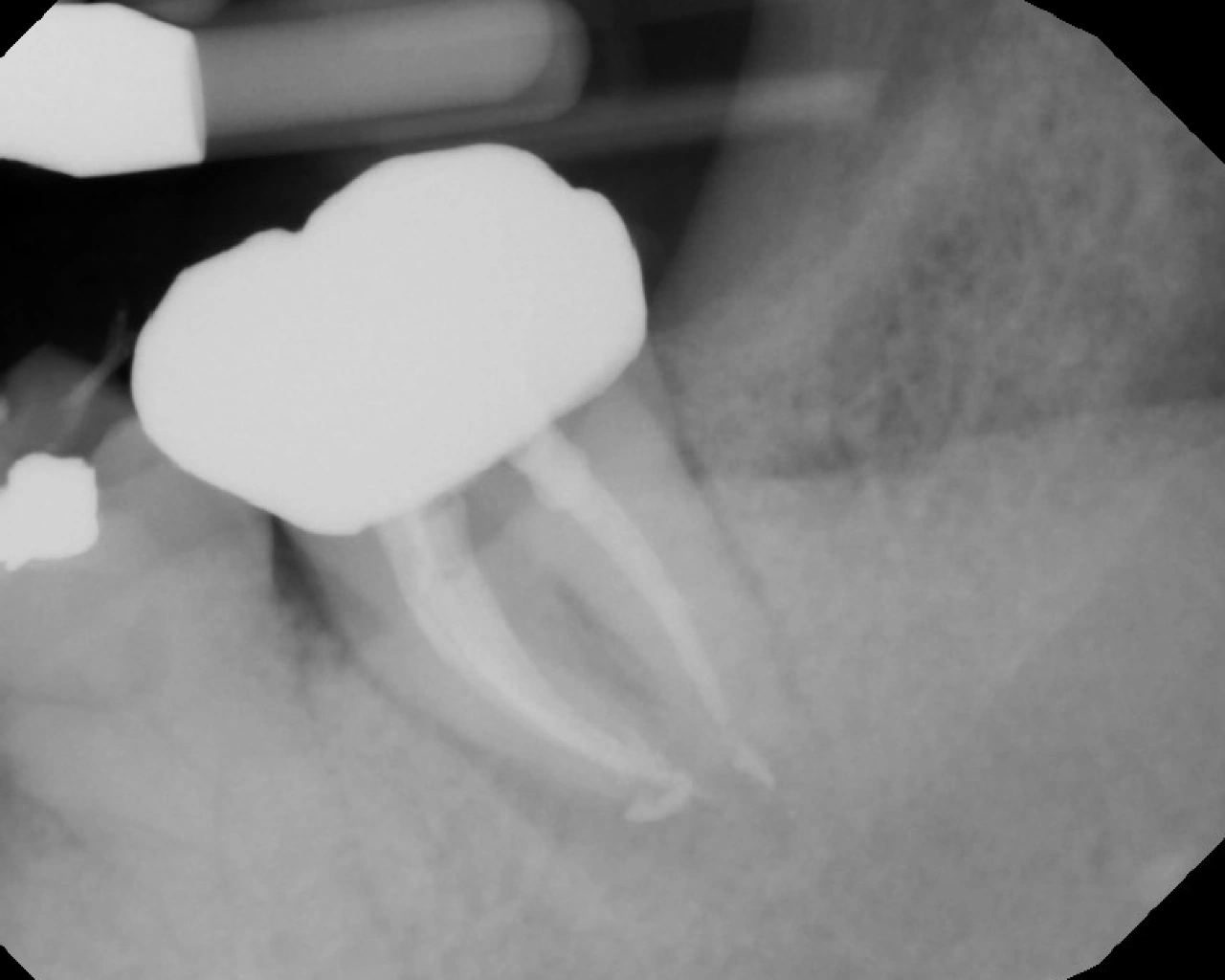
Master Cones

Obturation

Probing Depth in Buccal Furcation 5mm After Obturation

Core Build up
Zirconia Crown Cementation - 3 Months Later

Zirconia Crown Cementation - 3 Months Later
Tooth #18
A 56-year-old female patient presented with a chief complaint of swelling in the mandibular left posterior region. Clinical examination revealed a sinus tract located buccal to tooth #18. The sinus tract was traced using a gutta-percha cone, and radiographic evaluation demonstrated that the tract extended to the mesial root. Pulp vitality testing was non-responsive. The diagnosis was necrotic pulp with chronic apical abscess.
Root canal treatment was completed over three visits. During the first visit, an emergency pulpectomy was performed. The mesial canals were accessed and negotiated; however, the distal canals were extremely calcified and could not be fully explored due to time constraints. The canals were medicated and the tooth was temporized.
The second visit was completed in the postgraduate endodontic clinic with Dr. Haong using a dental operating microscope. The distal canals were carefully explored with EDTA and small hand files (#6, #8, and #10). A working length radiograph was obtained to confirm canal anatomy. The distal canals were instrumented using flexible rotary files with a 0.04 taper, while the mesial canals were prepared with WaveOne Gold Primary (Red). The sinus tract was still present and was retraced to the mesial canals. Irrigation was performed with sodium hypochlorite, saline, chlorhexidine, and EDTA. Internal fracture lines were noted within the chamber, and MTA was applied to seal the area. The canals were medicated with calcium hydroxide and the tooth was temporized.
At the third visit, resolution of the infection was noted, and the canals were obturated. Periodontal examination revealed deep probing in the furcation area, indicating an endo-perio lesion. The tooth has since been restored with a full-coverage crown, and follow-up evaluations are planned at 1-month, 3-month, and 6-month intervals to monitor healing.