RCT #18

Pre-Operative BW

Pre-Operative PA

Buccal Swelling

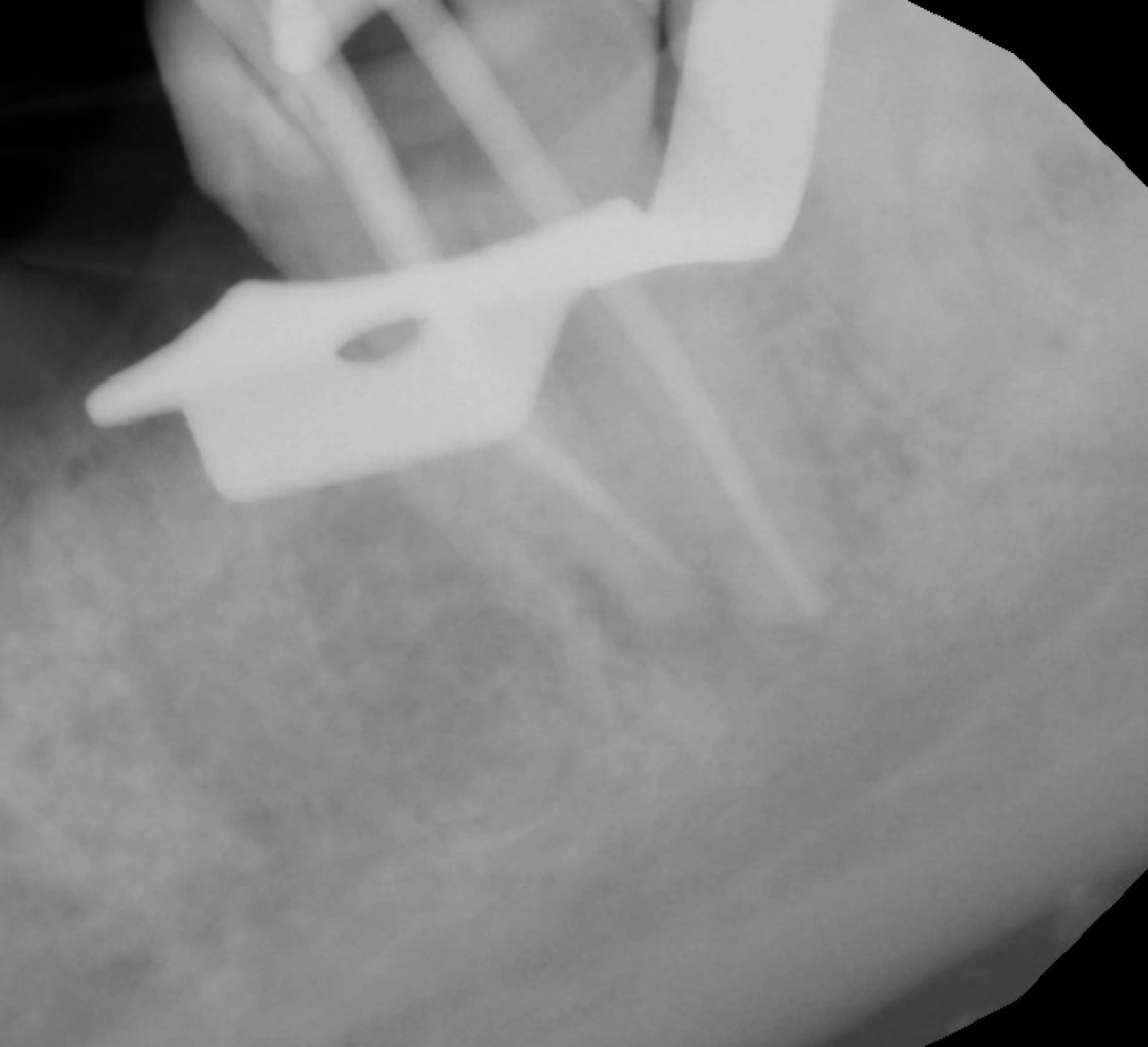
WL using size #8 and #10 files. (MB & ML meeting apically, and the apical constriction is offset to the distal)

Canals Instrumented
Master Cone, 1mm was cut from distal, and accessory cone was added

Obturation complete

IRM Applied
A 35-year-old female was referred by a colleague for root canal treatment on tooth #18. The referring provider had previously attempted vital pulp therapy; however, the patient later developed symptoms and experienced a flare-up, for which an emergency pulpotomy was performed by another provider.
At the patient’s initial visit for definitive root canal treatment, clinical examination revealed buccal swelling in the gingival tissue adjacent to the tooth. Pulp testing with Endo Ice was negative. The tooth exhibited mild tenderness to percussion and moderate tenderness to palpation. Based on the clinical and radiographic findings, the diagnosis was previously initiated therapy with chronic apical abscess.
During this visit, working length was established and the canals were instrumented using WaveOne Gold Primary (Red). Three canals were identified: mesiobuccal (MB), mesiolingual (ML), and distal. MB and ML canals join apically, and their apex is offset distally.
Distal canal was instrumented up to waveone medium, due to the large size of the canal, waveone large GP was selected, and 1.5mm was cut off to ensure proper apical fit. Both MB and ML were instrumented with waveone red and obturated with waveone red GP.